Single Inhaler Triple Therapy with Budesonide-Glycopyrronium-Formoterol fumarate in Uncontrolled Asthma



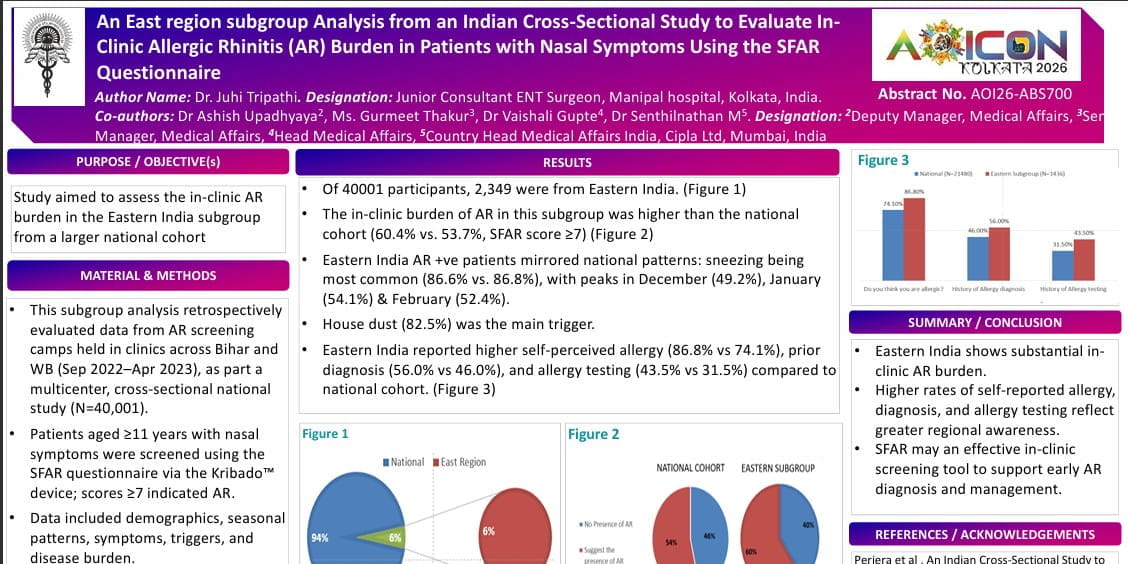
Introduction
Global Initiative for Asthma (GINA) recommends adding long‑acting muscarinic antagonist (LAMA) for uncontrolled asthma despite inhaled corticosteroid–long‑acting β₂‑agonist (ICS–LABA) maintenance therapy. Evidence has also shown that triple therapy with ICS-LAMA-LABA shows consistent improvement in lung function, but its effect on exacerbations has been unclear. A 2021 systematic review of five phase 3 trials found no significant reduction in severe exacerbations, partly due to study design and restricted populations with recent exacerbations. In contrast, the KALOS and LOGOS studies are the first to assess severe exacerbation risk in a broad representative asthma population, including individuals regardless of persistent airflow limitation or recent exacerbation history.
Aim
To assess the efficacy and safety of budesonide-glycopyrronium-formoterol fumarate dihydrate (BGF) versus budesonide-formoterol fumarate dihydrate (BFF) delivered via metered‑dose inhalers—either using co‑suspension technology (BFFA) or the current suspension formulation (BFFS)—in individuals with uncontrolled asthma.
Method
Study Design
- The KALOS and LOGOS studies were multicenter, randomized, double-blind, double-dummy, parallel group, phase 3 studies conducted over a treatment duration ranging from 24 to 52 weeks
- The participants were enrolled from 378 sites in 20 countries (KALOS), and 324 sites in 15 countries (LOGOS)
Patient Selection and Randomisation
- The study recruited individuals aged 12–80 years with inadequately controlled asthma despite receiving daily medium or high dose ICS–LABA therapy
- Participants were randomized into 4 groups who received the following inhalations twice daily via pressurized metered-dose inhaler for 24-52 weeks
- BGF 28·8 group - equivalent to budesonide 320 μg, glycopyrrolate 36 μg, and formoterol fumarate 9·6 μg
- BGF 14·4 group - equivalent to budesonide 320 μg, glycopyrrolate 18 μg, and formoterol fumarate 9·6 μg
- BFFA– budesonide 320 μg, formoterol fumarate 10 μg
- BFFS– budesonide 320 μg, formoterol fumarate 9 μg
- Cohort was followed up at weeks 4, 8, 12, 16, 20, 24, 28, 36, 44, and 52
Endpoints
Efficacy Endpoints
- Change from baseline in morning pre-dose trough FEV1from day 1 to week 24
- Change from baseline in FEV1area under the curve from 0 h to 3 h (AUC0-3) from day 1 to week 24
- Annualised rate of severe exacerbation
Safety Endpoints
- Incidence of adverse events (AEs)
Results
- Across the KALOS and LOGOS studies, n=4,311 received treatment
- BGF 28.8 μg significantly improved lung function (trough FEV₁ and FEV₁ AUC) versus all comparators as shown in Table 1.
Table 1. Lung function endpoints in the pooled KALOS and LOGOS studies
|
|
BGF 28.8 (n=1179) |
BGF 14.4 (n=725) |
BFFcombined (n=2400) |
|
Change from baseline in morning pre-dose trough FEV1 over 24 weeks (ml) |
|||
|
LS mean (SE) |
166 (8) |
156 (10) |
90 (6) |
|
LSM difference; p value |
76; <0.0001 |
65; <0.0001 |
Comparator |
|
Change from baseline in FEV1 AUC0-3 over 24 weeks (ml) |
|||
|
LS mean (SE) |
328 (8) |
319 (10) |
238 (5) |
|
LSM difference; p value |
90; <0.0001 |
81; <0.0001 |
Comparator |
LS – least squares
LSM – least square mean
- BGF 28·8 significantly reduced severe exacerbation rates versus BFFS [incidence rate ratio (IRR) 0·82; p=0·0043] and BFFcombined (IRR 0·86; p=0·012), but not versus BFFA (IRR 0·90; p=0·12)
- Time to first severe exacerbation favoured BGF 28·8 vs BFFS [Hazard ratio (HR) 0·81] and BFFcombined (HR 0·84), with non‑significant benefit vs BFFA (HR 0·88)
- Benefits persisted to week 52 for both BGF doses
- The incidence of AEs was similar across all treatment groups as shown in Figure 1.
Figure 1. Incidence of AEs

- No deaths related to treatment were reported
Conclusion
- Single‑inhaler triple therapy with budesonide-glycopyrronium-formoterol fumarate dihydrate (BGF) is superior to standard inhaled corticosteroid-long‑acting β₂‑agonist (ICS–LABA) in improving lung function and reducing exacerbations in patients aged 12–80 years with inadequately controlled asthma
- Benefits were observed across a broad population, including patients without a recent history of asthma exacerbations
Lancet Respir Med. 2026 Feb 12:S2213-2600(25)00457-6.